Perimenopause vs. Menopause: A Clinical Overview for Women Navigating the Hormonal Transition
The terms "perimenopause" and "menopause" are frequently used interchangeably, yet they represent distinct biological phases with different diagnostic criteria, hormonal profiles, and clinical management strategies.
Understanding this distinction is essential - not only for accurate diagnosis, but for initiating the right treatment at the right time, which has significant implications for a woman's long-term cardiovascular, skeletal, and cognitive health.
This article provides a clinically accurate review of both stages, the diagnostic approach recommended by current evidence-based guidelines, the full spectrum of symptoms beyond vasomotor complaints, and what the FDA's landmark 2025–2026 labeling revision means for women and their healthcare providers.
Menopause
Menopause is defined as the permanent cessation of menstruation resulting from the loss of ovarian follicular activity. Per ACOG Practice Bulletin No. 141 (reaffirmed 2024) and The Menopause Society, the clinical diagnosis requires 12 consecutive months of amenorrhea in the absence of other biological or physiological causes, in women over age 45. The average age of natural menopause in the United States is 51 years.
Menopause is a retrospective, single-point diagnosis - it cannot be confirmed until 12 months of amenorrhea have elapsed. It is not a process but a biological milestone. Everything prior to that point is the menopausal transition.
Perimenopause
(The Menopausal Transition)
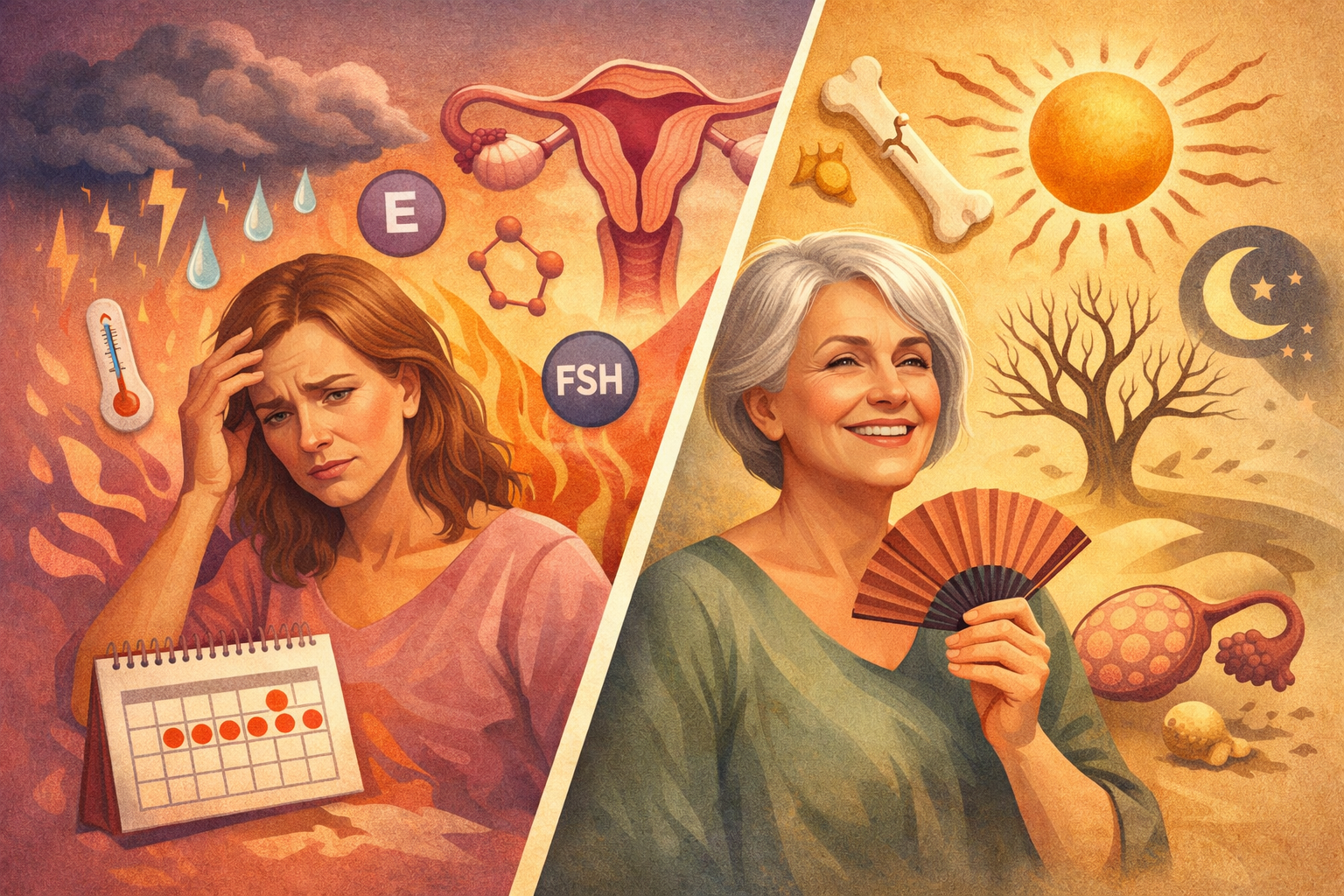
Perimenopause, also termed the menopausal transition, begins with variation in menstrual cycle length and a measurable rise in follicle-stimulating hormone (FSH), and ends with the final menstrual period (FMP). Using the Stages of Reproductive Aging Workshop (STRAW+10) framework — the internationally accepted staging system — perimenopause encompasses two phases:
- Early menopausal transition (STRAW −2): Menstrual cycle variability of ≥7 days difference from the normal cycle length on two or more occasions within 10 cycles. FSH begins rising.
- Late menopausal transition (STRAW −1): Amenorrhea of ≥60 days; FSH is consistently elevated; vasomotor symptoms are typically most pronounced during this stage.
This transition begins, on average, four to eight years before the final menstrual period and most commonly starts in the mid-to-late 40s, though it can begin in the late 30s.
A critical and clinically underappreciated point: perimenopause is not characterized by a steady decline in estrogen. In early perimenopause, estradiol levels can be supraphysiologic relative to a woman's prior baseline, driven by compensatory FSH hyperstimulation of the remaining ovarian follicles. It is this erratic hormonal volatility — peaks and precipitous drops — that generates much of the symptom burden, not estrogen deficiency per se. This distinction has direct implications for how and when to initiate therapy.
Symptom Profile: Beyond Vasomotor Symptoms
Hot flashes and night sweats (vasomotor symptoms, or VMS) are the most recognized manifestations of the menopausal transition, affecting approximately 75% of women.
However, the symptom profile of perimenopause and menopause extends across multiple organ systems, reflecting the broad distribution of estrogen receptors throughout the body - including the brain, cardiovascular system, musculoskeletal system, bladder, and skin.
Neurological and Cognitive Symptoms
Estrogen plays a significant modulatory role in the central nervous system. Estrogen receptors are expressed in the hypothalamus, hippocampus, prefrontal cortex, and amygdala - regions governing thermoregulation, memory consolidation, executive function, and mood. As estrogen signaling becomes erratic during perimenopause and then declines in postmenopause, several neurological manifestations commonly present:
- Cognitive changes: Difficulty with verbal recall, attention, and processing speed — often described as "brain fog" — affects up to 60% of women during the menopausal transition. These changes are neurobiologically mediated and have been associated with measurable reductions in brain metabolic activity on neuroimaging studies, particularly in the frontal and temporal cortices.
- Mood disturbances: Fluctuating estrogen alters serotonergic and noradrenergic neurotransmitter activity. New-onset anxiety, irritability, and low mood are common in perimenopause, even in women with no prior psychiatric history. The transition period carries an elevated risk for major depressive episodes compared to the premenopausal years.
- Sleep disruption: Beyond VMS-related awakenings, declining progesterone directly affects sleep architecture by reducing GABAergic activity. Many perimenopausal women experience difficulty maintaining sleep regardless of whether they have concurrent night sweats.
Cardiovascular Symptoms
- Palpitations: Reported by up to 40% of perimenopausal women. These are typically benign and attributable to estrogen's role in autonomic nervous system regulation and cardiac ion channel function. However, palpitations warrant appropriate cardiac evaluation to rule out structural or arrhythmic pathology before attributing them to the hormonal transition.
- Cardiovascular risk: Estrogen has well-established cardioprotective properties, including favorable effects on lipid profiles, endothelial function, and arterial compliance. As estrogen declines postmenopausally, cardiovascular risk rises significantly. Women who experience premature or surgical menopause face an accelerated risk trajectory.
Musculoskeletal Symptoms
Joint pain, morning stiffness, and myalgias are frequently reported during perimenopause and are attributable to estrogen's anti-inflammatory and chondroprotective properties. Additionally, accelerated bone loss begins during the late menopausal transition — up to 2–3% annually in the first several years following the FMP — substantially elevating fracture risk if not addressed.
Genitourinary Syndrome of Menopause (GSM)
GSM encompasses a constellation of vulvovaginal and lower urinary tract changes resulting from urogenital tissue atrophy in the setting of estrogen deficiency. Symptoms include vaginal dryness, dyspareunia, recurrent urinary tract infections, urinary urgency, and urge incontinence. Unlike vasomotor symptoms, GSM is a chronic, progressive condition that does not resolve without treatment. It affects approximately 50–70% of postmenopausal women and is significantly underreported due to patient reluctance to discuss it.
Diagnostic Approach: What Current Guidelines Recommend
Women Over Age 45
Per ACOG, The Menopause Society (formerly NAMS), and NICE NG23 (reviewed 2024), hormone level testing is generally not required to diagnose perimenopause or menopause in women aged 45 and older presenting with characteristic symptoms and menstrual irregularity. The diagnosis is clinical, based on age, symptom pattern, and menstrual history.
FSH testing in this age group is frequently misleading due to significant intra-cycle and inter-cycle variability during the early menopausal transition. A single FSH measurement within a normal premenopausal range does not exclude perimenopause.
Women Ages 40–45
In women aged 40–45 presenting with menopausal symptoms or menstrual irregularity, serum FSH measurement may be considered to support clinical diagnosis, though it remains not independently diagnostic. Per the European Society of Endocrinology (ESE) Clinical Practice Guideline (October 2025), if biochemical testing is pursued, FSH should be measured on days 2–5 of the menstrual cycle, or after an interval of more than 40 days without menstruation. Given FSH fluctuation, a second measurement 4–6 weeks later may be required.
Differential diagnoses to exclude in this age group include thyroid dysfunction (TSH), hyperprolactinemia, polycystic ovary syndrome (PCOS), and functional hypothalamic amenorrhea — all of which can produce overlapping symptom profiles.
Women Under Age 40
Amenorrhea and menopausal symptoms in women under 40 should prompt evaluation for Premature Ovarian Insufficiency (POI), a distinct diagnosis requiring its own management pathway. Diagnostic criteria per ESHRE guidelines include oligomenorrhea or amenorrhea for at least 4 months plus an elevated FSH greater than 25 IU/L on two occasions at least 4 weeks apart. POI carries substantial implications for bone health, cardiovascular risk, and fertility counseling, and warrants referral to a menopause specialist and, where appropriate, a multidisciplinary team.
The FDA's Landmark 2025–2026 Revision of Hormone Therapy Labeling
One of the most consequential policy changes in women's health in over two decades occurred in November 2025, when the U.S. Food and Drug Administration (FDA), together with the Department of Health and Human Services (HHS), announced the removal of broad black-box warnings from menopausal hormone therapy (HT) products.
Background: The Origins of the Black Box
The black-box warnings were applied to all estrogen-containing menopausal therapies in 2003, following the publication of early results from the Women's Health Initiative (WHI) — a large randomized controlled trial that suggested elevated risks of cardiovascular disease, breast cancer, stroke, and probable dementia associated with HT use. This prompted an immediate and dramatic decline in HT prescribing — by approximately 45% — and left millions of women undertreated for symptomatic menopause for more than two decades.
However, critical methodological limitations of the original WHI analysis were subsequently identified and extensively documented:
- The WHI study population had a mean participant age of 63 years — more than a decade older than the typical age of menopause onset and well outside the population for whom systemic HT is indicated.
- Many participants had pre-existing cardiovascular risk factors not representative of newly menopausal women.
- The progestogen used in the combined-therapy arm was medroxyprogesterone acetate (MPA) — a synthetic formulation not in common use today and one now recognized to carry a different risk profile than micronized progesterone or other progestogen formulations.
- The WHI dementia findings were derived exclusively from women aged 65–79 — again, not the target population initiating HT for vasomotor symptom management.
Subsequent reanalyses of WHI data in younger cohorts, combined with extensive observational data and randomized trial follow-up, produced a substantially different risk-benefit picture.
What the FDA Changed — and What Remains
Following a comprehensive review of the scientific literature, a formal expert panel convened in July 2025, and a public comment period, the FDA announced it would remove black-box warnings related to cardiovascular disease, breast cancer, and probable dementia from all HRT products used to treat menopausal symptoms. The labeling changes went into effect in February 2026.
The FDA also recommended removing the prior instruction to use "the lowest effective dose for the shortest possible duration" — language that had no evidence base and contributed to significant therapeutic undertreatment.
What the revised labeling now reflects:
Based on data from women who initiated HT within 10 years of menopause onset or before age 60:
- Up to 50% reduction in cardiovascular risk, including heart attack
- 35% reduction in risk of Alzheimer's disease
- 50–60% reduction in fracture risk
- 64% reduction in cognitive decline
- In a meta-analysis of 30 trials involving over 26,700 women, HT was not associated with increased cancer mortality
Updated labels will be rewritten with age-specific guidance indicating that women may reap long-term health benefits if hormone therapy is initiated within 10 years of menopause onset.
What remains unchanged:
- The black-box warning for endometrial cancer on systemic estrogen-alone products in women with an intact uterus is retained. Systemic estrogen-alone therapy requires concurrent progestogen in women who have not had a hysterectomy.
- Women with a personal or family history of hormone-sensitive breast cancer require individualized risk-benefit discussion, ideally in coordination with oncology, as the risk and benefit considerations differ meaningfully from the general menopausal population.
- Vaginal estrogen products carry minimal systemic absorption, and FDA panelists specifically pushed to remove or revise the boxed warning on vaginal estrogen because only minimal amounts of estrogen are absorbed from the vagina into the bloodstream.
The FDA's decision does not represent a blanket endorsement of hormone therapy for all menopausal women. It represents a restoration of evidence-based, individualized clinical decision-making — free from the distortion introduced by a misapplied, 23-year-old warning label.
Current Treatment Framework
Hormone Therapy: Formulation and Route Matter
Not all hormone therapy formulations carry equivalent risk-benefit profiles. Clinical decision-making around HT requires individualization based on a woman's symptom burden, age, time since menopause onset, and personal and family medical history.
Key distinctions supported by current evidence:
- Transdermal estradiol (patch, gel, spray) has a more favorable thrombotic risk profile than oral conjugated equine estrogens (CEE), because transdermal delivery bypasses first-pass hepatic metabolism and does not increase clotting factor synthesis or C-reactive protein to the same degree.
- Micronized progesterone (bioidentical) appears to carry a lower association with breast cancer and adverse cardiovascular effects than synthetic medroxyprogesterone acetate, based on data from the French E3N cohort study and subsequent analyses.
- Timing of initiation is clinically significant. The "timing hypothesis" — supported by substantial data — indicates that cardiovascular and neuroprotective benefits of HT are greatest when initiated during perimenopause or within 10 years of the final menstrual period, and in a vascular system that has not yet undergone significant atherosclerotic or neurological change.
- Low-dose vaginal estrogen for GSM carries negligible systemic absorption and is appropriate for the majority of menopausal women, including many with a history of estrogen-sensitive malignancies — a decision made with oncologic input.
Per The Menopause Society and ACOG, the current recommendation does not support routine use of compounded, non-FDA-approved hormone preparations as a first-line approach. FDA-approved bioidentical formulations (including transdermal estradiol and oral micronized progesterone) are available, regulated for potency and purity, and represent the evidence-based standard of care.
Non-Hormonal Pharmacologic Options
For women who are not candidates for systemic hormone therapy or who prefer to avoid it, multiple evidence-based non-hormonal options are available:
- Fezolinetant (Veozah®): FDA-approved in 2023 as the first non-hormonal treatment specifically targeting the hypothalamic thermoregulatory pathway via NK3 receptor antagonism. Clinical trials demonstrated significant reductions in VMS frequency and severity.
- Elinzanetant: A dual NK1/NK3 receptor antagonist in late-stage trials as of 2025, showing promising results for VMS and sleep disruption. (JAMA Internal Medicine, September 2025)
- SSRIs/SNRIs: Paroxetine (Brisdelle®, FDA-approved for VMS), venlafaxine, and escitalopram have demonstrated efficacy for both vasomotor symptoms and mood disturbance in menopausal women.
- Gabapentin: Modestly effective for VMS and sleep disruption; appropriate in select patients.
Lifestyle and Preventive Strategies
Irrespective of pharmacologic therapy, several evidence-supported lifestyle interventions meaningfully affect long-term outcomes during the menopausal transition:
- Progressive resistance training is the most impactful modifiable intervention for preserving bone mineral density, maintaining skeletal muscle mass, and improving metabolic parameters during menopause.
- Cardiovascular exercise supports endothelial function, lipid management, and sleep quality.
- Dietary optimization — including adequate calcium (1,200 mg/day postmenopausally), vitamin D (1,500–2,000 IU/day), and reduced ultra-processed food intake — addresses both bone and cardiovascular risk.
Alcohol reduction: Alcohol amplifies vasomotor symptom frequency and is associated with increased breast cancer risk; reduction is clinically advisable.
When to Seek Evaluation
Women in the menopausal transition should not delay seeking evaluation. The perimenopausal window represents a critical period for preventive intervention — decisions made during this phase have implications that extend well beyond symptom relief.
Evaluation is appropriate when any of the following are present:
- Menstrual irregularity in women over 40, particularly cycles shorter than 21 days or longer than 45 days
- New onset of vasomotor symptoms, sleep disruption, cognitive changes, or mood disturbance
- Genitourinary symptoms including vaginal dryness, recurrent UTIs, or urinary urgency
- Bleeding after 12 months of amenorrhea (requires prompt evaluation to exclude endometrial pathology)
- Menopausal symptoms in women under 40 (requires POI workup)
- Interest in understanding candidacy for hormone therapy or non-hormonal alternatives
Conclusion
Perimenopause and menopause are not interchangeable diagnoses, and the distinctions between them carry direct clinical consequences. The menopausal transition begins years before the final menstrual period and involves complex hormonal dynamics that affect nearly every organ system.
The FDA's November 2025 removal of broad black-box warnings from hormone therapy products reflects more than two decades of accumulated evidence correcting the misapplication of early WHI data -and signals a return to individualized, evidence-based care for women navigating this transition.
Early, expert evaluation allows for accurate staging, appropriate diagnostic workup where indicated, and timely initiation of treatment during the window in which long-term protective benefits are most pronounced.
References
- ACOG Practice Bulletin No. 141: Management of Menopausal Symptoms. Obstet Gynecol. 2014 (reaffirmed 2024).
- The Menopause Society (NAMS). 2022 Hormone Therapy Position Statement. Menopause. 2022;29(7):767–794.
- Lumsden MA, et al. European Society of Endocrinology Clinical Practice Guideline for Evaluation and Management of Menopause and the Perimenopause. Eur J Endocrinol. 2025;193(4):G49–G81. https://doi.org/10.1093/ejendo/lvaf206
- Makary MA, Nguyen CP, Høeg TB, Tidmarsh GF. Updated Labeling for Menopausal Hormone Therapy. JAMA. 2026;335(2):117–118. doi:10.1001/jama.2025.22259
- HHS/FDA. HHS Advances Women's Health, Removes Misleading FDA Warnings on Hormone Replacement Therapy. Press Release. November 10, 2025. https://www.fda.gov/news-events/press-announcements/hhs-advances-womens-health-removes-misleading-fda-warnings-hormone-replacement-therapy
- FDA. FDA Approves Labeling Changes to Menopausal Hormone Therapy Products. February 12, 2026. https://www.fda.gov
- Soules MR, et al. Stages of Reproductive Aging Workshop (STRAW). Fertil Steril. 2001;76(5):874–878. (STRAW+10 update: Harlow et al., Menopause. 2012)
- NICE Guideline NG23: Menopause — Identification and Management. Last reviewed November 2024. https://www.nice.org.uk/guidance/ng23
- Panay N, Joffe H, Maki PM, et al. Elinzanetant for the Treatment of Vasomotor Symptoms Associated With Menopause: A Phase 3 Randomized Clinical Trial. JAMA Intern Med. 2025 Sep 8.
- Agrawal P, et al. Safety of Vaginal Estrogen Therapy for Genitourinary Syndrome of Menopause in Women With a History of Breast Cancer. Obstet Gynecol. 2023;142(3):660–668.
This content is intended for educational and informational purposes only. It does not constitute individualized medical advice and is not a substitute for consultation with a qualified gynecologist or healthcare provider. All treatment decisions should be made in the context of a complete clinical evaluation and the patient's individual health history.
Content reviewed and approved by Hema Jonnalagadda, MD, FACOG, Member of The Menopause Society | Advocare Montgomery Gynecology, Plymouth Meeting, PA | 215-444-3411
Bleeding Menstrual: What is Normal and What is Abnormal
Menstrual bleeding, or menstruation, is a complex physiological process that involves the shedding of the endometrial lining of the uterus. This guide, formulated with insights from Dr. Hema Jonnalagadda, aims to provide an exhaustive, scientifically detailed overview of normal and abnormal menstrual bleeding. This resource will address every aspect of menstrual health, offering comprehensive knowledge to clarify all potential queries.

Menstrual Cycle Phases: A Detailed Breakdown with Simplified Clarifications
The menstrual cycle is regulated by a finely tuned interplay of hormones. It is typically divided into four phases:
Menstrual Phase (Days 1-5)
● Pathophysiology: Shedding of the functional layer of the endometrium due to the drop in progesterone levels.
- Simplified Clarification: The uterine lining breaks down and is expelled as menstrual blood due to lower hormone levels.
● Normal Findings: Bleeding lasting 3-7 days with a total blood loss of 30-80 milliliters.
- Simplified Clarification: Menstruation typically lasts 3-7 days, with an average blood loss of 2-6 tablespoons.
Follicular Phase (Days 1-13)
● Endocrine Regulation: Increased secretion of Follicle Stimulating Hormone (FSH) from the anterior pituitary stimulates follicular growth.
- Simplified Clarification: The brain signals the ovaries to start maturing eggs.
● Endometrial Changes: Proliferation of the endometrium due to rising estrogen levels.
- Simplified Clarification: The uterine lining thickens and rebuilds.
Ovulation (Day 14)
● Hormonal Surge: A peak in Luteinizing Hormone (LH) triggers the release of a mature oocyte.
- Simplified Clarification: A spike in a specific hormone causes an egg to be released from the ovary.
● Clinical Significance: Mid-cycle pain (Mittelschmerz) may be observed, and cervical mucus becomes more elastic and clear, facilitating sperm entry.
- Simplified Clarification: Some women feel slight pain during ovulation, and cervical mucus changes to help sperm reach the egg.
Luteal Phase (Days 15-28)
● Hormonal Influence: The corpus luteum secretes progesterone, stabilizing the endometrial lining for potential implantation.
- Simplified Clarification: The body produces a hormone to keep the uterine lining ready for a potential pregnancy.
● Endometrial Maturation: Glandular secretion and increased vascularization of the endometrium.
- Simplified Clarification: The uterine lining becomes nutrient-rich and full of blood vessels to support a possible pregnancy.
Normal Menstrual Bleeding: Clinical and Pathological Insights
Duration and Volume:
● Clinical Norms: Menstrual bleeding lasting between 3-7 days, with an average blood loss of 30-80 milliliters.
● Measurement Techniques: The use of menstrual cups or calibrated sanitary products can aid in quantifying blood loss.

Color and Consistency:
● Hemoglobin Breakdown: Initial bright red bleeding progressing to darker red or brown due to oxidation.
● Clot Formation: Small clots are normal; large clots may indicate excessive bleeding or an underlying coagulopathy.
Cycle Regularity:
● Eumenorrhea: Regular cycles ranging from 21 to 35 days.
● Variations: Minor deviations are normal but should be monitored if consistent irregularities occur.
Abnormal Menstrual Bleeding (AUB): Etiologies and Diagnostics
Abnormal uterine bleeding (AUB) can be a symptom of various underlying pathologies. The International Federation of Gynecology and Obstetrics (FIGO) classifies AUB into structural and non-structural causes using the PALM-COEIN system:
Structural Causes (PALM)
- Polyp : Endometrial or cervical polyps causing irregular bleeding.
- Simplified Clarification : Non-cancerous growths in the uterus or cervix that can cause unusual bleeding.
- Adenomyosis : Invasion of endometrial tissue into the myometrium, resulting in heavy, painful periods.
- Simplified Clarification : When the lining of the uterus grows into the muscle wall, causing heavy and painful periods.
- Leiomyoma (Fibroids) : Benign uterine tumors causing menorrhagia and pressure symptoms.
- Simplified Clarification : Non-cancerous tumors in the uterus that cause heavy bleeding and a feeling of pressure.
- Malignancy and Hyperplasia : Endometrial hyperplasia and cancer presenting with postmenopausal bleeding or irregular heavy bleeding.
- Simplified Clarification : Thickening of the uterine lining or cancer, which can cause unusual heavy bleeding, especially after menopause.
Non-Structural Causes (COEIN)
- Coagulopathy : Conditions such as von Willebrand disease leading to excessive bleeding.
- Simplified Clarification : Blood clotting disorders that cause too much bleeding.
- Ovulatory Dysfunction: Irregular ovulation causing unpredictable bleeding patterns.
- Simplified Clarification : Irregular ovulation leading to unpredictable menstrual cycles.
- Endometrial : Primary endometrial dysfunction without a definable structural cause.
- Simplified Clarification : Issues with the uterine lining that aren't caused by growths or other structural problems.
- Iatrogenic : Medications or devices (e.g., IUDs) leading to abnormal bleeding.
- Simplified Clarification : Certain medications or medical devices can cause unusual bleeding.
- Not Yet Classified : Cases where the etiology remains unclear.
- Simplified Clarification : Causes of abnormal bleeding that haven't been identified yet.
Heavy Menstrual Bleeding (Menorrhagia)
● Pathophysiology: Often due to uterine fibroids, adenomyosis, or coagulopathies.
● Clinical Assessment: Laboratory evaluation (CBC, coagulation profile), imaging (ultrasound, MRI), and endometrial biopsy as needed.
Intermenstrual Bleeding
● Etiologies: Can result from hormonal contraception, infections, or structural abnormalities.
● Diagnostics: Pap smear, pelvic ultrasound, and hysteroscopy.
Postmenopausal Bleeding
● Red Flags: Requires immediate investigation to rule out endometrial carcinoma.
● Investigative Protocols: Transvaginal ultrasound and endometrial biopsy.
Light Menstrual Bleeding (Hypomenorrhea)
● Causes: Hormonal contraception, chronic medical conditions, or Asherman’s syndrome.
● Management: Hormonal assessment, hysteroscopy for intrauterine adhesions.
Infrequent Menstrual Bleeding (Oligomenorrhea)
● Common Causes: PCOS, thyroid dysfunction, hyperprolactinemia.
● Evaluation: Hormonal profile, pelvic ultrasound, and MRI of the pituitary gland if necessary.
Frequent Menstrual Bleeding (Polymenorrhea)
● Considerations: Hormonal imbalances, endometrial pathology.
● Assessment: Endocrine evaluation, endometrial sampling.
Painful Menstrual Bleeding (Dysmenorrhea)
● Primary: Excessive prostaglandin production leading to uterine contractions.
● Secondary: Endometriosis, fibroids, or pelvic inflammatory disease (PID).
● Management: NSAIDs, hormonal treatments, laparoscopic evaluation for endometriosis.
Diagnostic and Therapeutic Approaches
Diagnostic Tools
● Transvaginal Ultrasound: Gold standard for evaluating endometrial and myometrial pathology.
● Saline Infusion Sonography (SIS): Enhances the evaluation of intrauterine pathology.
● MRI: Detailed imaging for complex cases, especially adenomyosis or deep infiltrating endometriosis.
● Hysteroscopy: Direct visualization and biopsy of intrauterine lesions.
● Endometrial Biopsy: Essential for ruling out hyperplasia or malignancy.
Treatment Modalities
● Medical Management:
- Hormonal Therapy: Combined oral contraceptives, progestins, GnRH analogs.
- Non-Hormonal: NSAIDs, antifibrinolytics like tranexamic acid.
● Surgical Interventions:
- Dilation and Curettage (D&C): For diagnostic and therapeutic purposes.
- Endometrial Ablation: Minimally invasive treatment for menorrhagia.
- Myomectomy: Removal of fibroids preserving the uterus.
- Hysterectomy: Definitive treatment for refractory AUB, especially in the context of malignancy.
Lifestyle and Supportive Measures
● Dietary Modifications: Iron-rich diet to combat anemia, balanced nutrition to maintain hormonal balance.
● Exercise: Regular physical activity to manage weight and reduce stress.
● Stress Management: Techniques like mindfulness, yoga, and counseling.
Conclusion
A thorough understanding of normal and abnormal menstrual bleeding patterns is vital for early detection and management of underlying gynecological disorders. This comprehensive guide serves as an exhaustive resource to demystify menstrual health, providing detailed scientific insights and practical approaches to managing various menstrual disorders.
Advocare Montgomery Gynecology, located in Plymouth Meeting, offers comprehensive care for women's health needs. Many procedures for diagnosing and treating menstrual disorders can be conveniently performed in-office, while others may require specialized referrals. Selecting the right practitioner at the right time is crucial for effective treatment. At Advocare Montgomery Gynecology, Dr. Hema Jonnalagadda and her experienced team are dedicated to offering expert, compassionate care tailored to your individual needs.
For personalized medical advice and treatment, consult with Dr. Hema Jonnalagadda and the team at Advocare Montgomery Gynecology. We have the expertise and resources to help you manage your menstrual health with confidence and ease.
For further information or to schedule an appointment, please visit our [website](https://www.advocaremontgomerygyn.com/).
Choose Advocare Montgomery Gynecology for exceptional care and support on your journey to optimal gynecological health.