Bleeding Menstrual: What is Normal and What is Abnormal
Menstrual bleeding, or menstruation, is a complex physiological process that involves the shedding of the endometrial lining of the uterus. This guide, formulated with insights from Dr. Hema Jonnalagadda, aims to provide an exhaustive, scientifically detailed overview of normal and abnormal menstrual bleeding. This resource will address every aspect of menstrual health, offering comprehensive knowledge to clarify all potential queries.
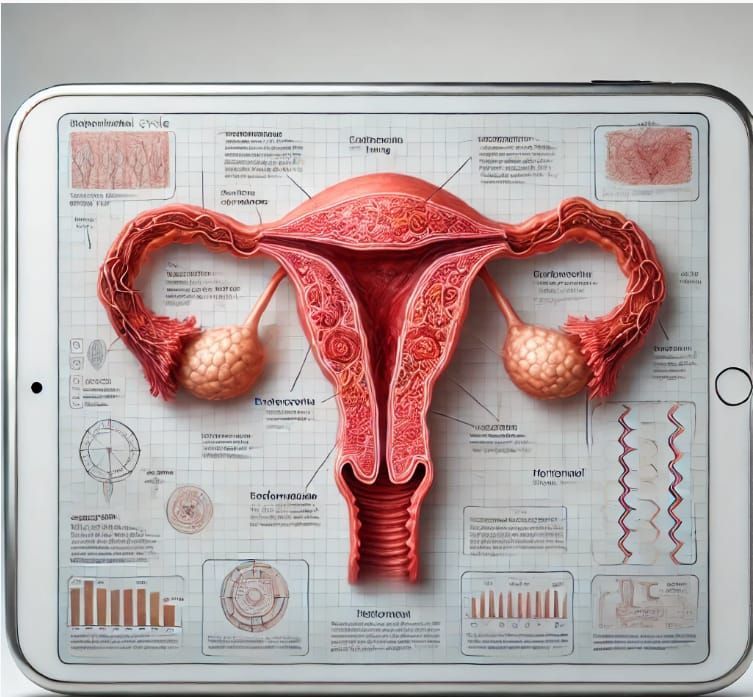

Menstrual Cycle Phases: A Detailed Breakdown with Simplified Clarifications
The menstrual cycle is regulated by a finely tuned interplay of hormones. It is typically divided into four phases:
Menstrual Phase (Days 1-5)
● Pathophysiology: Shedding of the functional layer of the endometrium due to the drop in progesterone levels.
- Simplified Clarification: The uterine lining breaks down and is expelled as menstrual blood due to lower hormone levels.
● Normal Findings: Bleeding lasting 3-7 days with a total blood loss of 30-80 milliliters.
- Simplified Clarification: Menstruation typically lasts 3-7 days, with an average blood loss of 2-6 tablespoons.
Follicular Phase (Days 1-13)
● Endocrine Regulation: Increased secretion of Follicle Stimulating Hormone (FSH) from the anterior pituitary stimulates follicular growth.
- Simplified Clarification: The brain signals the ovaries to start maturing eggs.
● Endometrial Changes: Proliferation of the endometrium due to rising estrogen levels.
- Simplified Clarification: The uterine lining thickens and rebuilds.
Ovulation (Day 14)
● Hormonal Surge: A peak in Luteinizing Hormone (LH) triggers the release of a mature oocyte.
- Simplified Clarification: A spike in a specific hormone causes an egg to be released from the ovary.
● Clinical Significance: Mid-cycle pain (Mittelschmerz) may be observed, and cervical mucus becomes more elastic and clear, facilitating sperm entry.
- Simplified Clarification: Some women feel slight pain during ovulation, and cervical mucus changes to help sperm reach the egg.
Luteal Phase (Days 15-28)
● Hormonal Influence: The corpus luteum secretes progesterone, stabilizing the endometrial lining for potential implantation.
- Simplified Clarification: The body produces a hormone to keep the uterine lining ready for a potential pregnancy.
● Endometrial Maturation: Glandular secretion and increased vascularization of the endometrium.
- Simplified Clarification: The uterine lining becomes nutrient-rich and full of blood vessels to support a possible pregnancy.
Normal Menstrual Bleeding: Clinical and Pathological Insights
Duration and Volume:
● Clinical Norms: Menstrual bleeding lasting between 3-7 days, with an average blood loss of 30-80 milliliters.
● Measurement Techniques: The use of menstrual cups or calibrated sanitary products can aid in quantifying blood loss.

Color and Consistency:
● Hemoglobin Breakdown: Initial bright red bleeding progressing to darker red or brown due to oxidation.
● Clot Formation: Small clots are normal; large clots may indicate excessive bleeding or an underlying coagulopathy.
Cycle Regularity:
● Eumenorrhea: Regular cycles ranging from 21 to 35 days.
● Variations: Minor deviations are normal but should be monitored if consistent irregularities occur.
Abnormal Menstrual Bleeding (AUB): Etiologies and Diagnostics
Abnormal uterine bleeding (AUB) can be a symptom of various underlying pathologies. The International Federation of Gynecology and Obstetrics (FIGO) classifies AUB into structural and non-structural causes using the PALM-COEIN system:
Structural Causes (PALM)
- Polyp : Endometrial or cervical polyps causing irregular bleeding.
- Simplified Clarification : Non-cancerous growths in the uterus or cervix that can cause unusual bleeding.
- Adenomyosis : Invasion of endometrial tissue into the myometrium, resulting in heavy, painful periods.
- Simplified Clarification : When the lining of the uterus grows into the muscle wall, causing heavy and painful periods.
- Leiomyoma (Fibroids) : Benign uterine tumors causing menorrhagia and pressure symptoms.
- Simplified Clarification : Non-cancerous tumors in the uterus that cause heavy bleeding and a feeling of pressure.
- Malignancy and Hyperplasia : Endometrial hyperplasia and cancer presenting with postmenopausal bleeding or irregular heavy bleeding.
- Simplified Clarification : Thickening of the uterine lining or cancer, which can cause unusual heavy bleeding, especially after menopause.
Non-Structural Causes (COEIN)
- Coagulopathy : Conditions such as von Willebrand disease leading to excessive bleeding.
- Simplified Clarification : Blood clotting disorders that cause too much bleeding.
- Ovulatory Dysfunction: Irregular ovulation causing unpredictable bleeding patterns.
- Simplified Clarification : Irregular ovulation leading to unpredictable menstrual cycles.
- Endometrial : Primary endometrial dysfunction without a definable structural cause.
- Simplified Clarification : Issues with the uterine lining that aren't caused by growths or other structural problems.
- Iatrogenic : Medications or devices (e.g., IUDs) leading to abnormal bleeding.
- Simplified Clarification : Certain medications or medical devices can cause unusual bleeding.
- Not Yet Classified : Cases where the etiology remains unclear.
- Simplified Clarification : Causes of abnormal bleeding that haven't been identified yet.
Heavy Menstrual Bleeding (Menorrhagia)
● Pathophysiology: Often due to uterine fibroids, adenomyosis, or coagulopathies.
● Clinical Assessment: Laboratory evaluation (CBC, coagulation profile), imaging (ultrasound, MRI), and endometrial biopsy as needed.
Intermenstrual Bleeding
● Etiologies: Can result from hormonal contraception, infections, or structural abnormalities.
● Diagnostics: Pap smear, pelvic ultrasound, and hysteroscopy.
Postmenopausal Bleeding
● Red Flags: Requires immediate investigation to rule out endometrial carcinoma.
● Investigative Protocols: Transvaginal ultrasound and endometrial biopsy.
Light Menstrual Bleeding (Hypomenorrhea)
● Causes: Hormonal contraception, chronic medical conditions, or Asherman’s syndrome.
● Management: Hormonal assessment, hysteroscopy for intrauterine adhesions.
Infrequent Menstrual Bleeding (Oligomenorrhea)
● Common Causes: PCOS, thyroid dysfunction, hyperprolactinemia.
● Evaluation: Hormonal profile, pelvic ultrasound, and MRI of the pituitary gland if necessary.
Frequent Menstrual Bleeding (Polymenorrhea)
● Considerations: Hormonal imbalances, endometrial pathology.
● Assessment: Endocrine evaluation, endometrial sampling.
Painful Menstrual Bleeding (Dysmenorrhea)
● Primary: Excessive prostaglandin production leading to uterine contractions.
● Secondary: Endometriosis, fibroids, or pelvic inflammatory disease (PID).
● Management: NSAIDs, hormonal treatments, laparoscopic evaluation for endometriosis.
Diagnostic and Therapeutic Approaches
Diagnostic Tools
● Transvaginal Ultrasound: Gold standard for evaluating endometrial and myometrial pathology.
● Saline Infusion Sonography (SIS): Enhances the evaluation of intrauterine pathology.
● MRI: Detailed imaging for complex cases, especially adenomyosis or deep infiltrating endometriosis.
● Hysteroscopy: Direct visualization and biopsy of intrauterine lesions.
● Endometrial Biopsy: Essential for ruling out hyperplasia or malignancy.
Treatment Modalities
● Medical Management:
- Hormonal Therapy: Combined oral contraceptives, progestins, GnRH analogs.
- Non-Hormonal: NSAIDs, antifibrinolytics like tranexamic acid.
● Surgical Interventions:
- Dilation and Curettage (D&C): For diagnostic and therapeutic purposes.
- Endometrial Ablation: Minimally invasive treatment for menorrhagia.
- Myomectomy: Removal of fibroids preserving the uterus.
- Hysterectomy: Definitive treatment for refractory AUB, especially in the context of malignancy.
Lifestyle and Supportive Measures
● Dietary Modifications: Iron-rich diet to combat anemia, balanced nutrition to maintain hormonal balance.
● Exercise: Regular physical activity to manage weight and reduce stress.
● Stress Management: Techniques like mindfulness, yoga, and counseling.
Conclusion
A thorough understanding of normal and abnormal menstrual bleeding patterns is vital for early detection and management of underlying gynecological disorders. This comprehensive guide serves as an exhaustive resource to demystify menstrual health, providing detailed scientific insights and practical approaches to managing various menstrual disorders.
Advocare Montgomery Gynecology, located in Plymouth Meeting, offers comprehensive care for women's health needs. Many procedures for diagnosing and treating menstrual disorders can be conveniently performed in-office, while others may require specialized referrals. Selecting the right practitioner at the right time is crucial for effective treatment. At Advocare Montgomery Gynecology, Dr. Hema Jonnalagadda and her experienced team are dedicated to offering expert, compassionate care tailored to your individual needs.
For personalized medical advice and treatment, consult with Dr. Hema Jonnalagadda and the team at Advocare Montgomery Gynecology. We have the expertise and resources to help you manage your menstrual health with confidence and ease.
For further information or to schedule an appointment, please visit our [website](https://www.advocaremontgomerygyn.com/).
Choose Advocare Montgomery Gynecology for exceptional care and support on your journey to optimal gynecological health.
A Note from Dr. Jonnalagadda
"Every woman I see with menopausal symptoms has a unique hormonal fingerprint, a unique health history, and a unique life. My job is not to hand you a one-size-fits-all prescription - it's to partner with you to build a treatment plan that fits your body, your goals, and your peace of mind. This article reflects how I think about HRT in my practice today."
If you've Googled "is HRT safe" at midnight while lying awake with your third hot flash of the evening, you're in good company. Millions of American women are navigating perimenopause and menopause with outdated information - much of it born from a single controversial study published over two decades ago that was widely misinterpreted and has since been substantially revised.
The good news: the science has caught up. The medical consensus in 2026 - from the Menopause Society, ACOG (American College of Obstetricians and Gynecologists), and leading research institutions worldwide - is more reassuring than it's been in years. For most healthy women who start treatment at the right time, HRT is not only safe - it may be the single most effective intervention for both symptom relief and long-term health preservation.
This guide is written by Dr. Hema Jonnalagadda, MD, board-certified gynecologist, founding physician of Advocare Montgomery Gynecology in Plymouth Meeting, Pennsylvania, and member of the Menopause Society. It covers everything you need to make an informed, confident decision - in language your body (and your schedule) can actually use.
1. What Is Hormone Replacement Therapy?
Hormone Replacement Therapy - also called Menopausal Hormone Therapy (MHT) in current clinical literature - is the medical replenishment of hormones that your body gradually stops producing as you approach and enter menopause. Primarily, this means estrogen, which is the dominant female sex hormone, and progesterone (or its synthetic counterpart, progestin), which protects the uterine lining from overgrowth caused by estrogen alone.
Some women also benefit from the addition of low-dose testosterone, which plays a largely unappreciated role in female libido, muscle mass, energy, and cognitive sharpness.
HRT comes in many forms: patches, gels, pills, sprays, vaginal rings, pellets, and creams. The delivery method matters - and choosing the right one is part of the personalized consultation that Dr. Jonnalagadda provides at Montgomery Gynecology.
2. The Science of Menopause & Hormonal Decline
Menopause is defined as 12 consecutive months without a menstrual period. The average American woman reaches menopause at age 51, though the transition - called perimenopause - can begin 8–10 years earlier, often in the early-to-mid 40s.
During perimenopause, your ovaries begin producing erratic, declining levels of estrogen and progesterone. This hormonal volatility - not the absence of hormones, but their unpredictability - is responsible for many of the most disruptive symptoms: irregular periods, mood swings, brain fog, and sleep disruption.
After menopause, estrogen levels drop to about one-tenth of their premenopausal levels. This isn't merely a reproductive shift - estrogen has receptors throughout the brain, heart, bones, skin, gut, bladder, and vaginal tissue. Its sustained decline has measurable effects on all of these systems over time.
What Estrogen Actually Does in Your Body
Most women are surprised to learn how far estrogen's influence extends beyond reproduction:
- Brain & Cognition: Supports neurotransmitter production, memory consolidation, and neuroprotection.
- Cardiovascular: Keeps blood vessels flexible and helps maintain healthy cholesterol ratios.
- Bone Density: Inhibits bone-resorbing cells; its decline is the #1 driver of postmenopausal osteoporosis.
- Vaginal & Urinary: Maintains mucosal integrity and prevents genitourinary syndrome of menopause (GSM).
- Sleep: Regulates thermostat function and supports deep, restorative sleep cycles.
- Skin & Collagen: Women lose up to 30% of skin collagen in the first 5 years after menopause.
3. Symptoms That Signal You May Need HRT
The decision to consider HRT begins with your symptoms - their severity, frequency, and impact on your daily life. At Montgomery Gynecology, Dr. Jonnalagadda uses a validated symptom-scoring tool at your first visit so that treatment decisions are based on objective data, not guesswork.
Common symptoms that drive women to seek HRT consultation include:
- Vasomotor symptoms: hot flashes, night sweats (affect 75–80% of menopausal women)
- Sleep disruption: difficulty falling or staying asleep, non-restorative sleep
- Genitourinary syndrome of menopause (GSM): vaginal dryness, painful intercourse, recurrent UTIs, urinary urgency
- Mood changes: irritability, anxiety, low mood, emotional volatility
- Cognitive symptoms: brain fog, difficulty concentrating, word-finding trouble
- Musculoskeletal: joint aches, muscle stiffness, fatigue
- Sexual dysfunction: decreased libido, difficulty with arousal or orgasm
- Changes in body composition: weight gain around the abdomen, loss of muscle tone
Important
These symptoms are common - but they are never "just menopause" that you have to endure. Effective, individualized treatment exists. You deserve to feel well at every stage of life, not merely survive it.
4. Types of HRT: Conventional vs. FDA-Approved Bioidentical
One of the most frequent questions Dr. Jonnalagadda receives is: "What's the difference between regular hormones and bioidentical hormones?" The answer requires separating marketing language from medical science.
FDA-Approved Bioidentical Hormones (Recommended)
Bioidentical means the hormone molecule is structurally identical to what your ovaries produce. FDA-approved bioidentical options include 17β-estradiol (patches, gels, sprays, vaginal rings) and micronized progesterone (Prometrium®). These have been rigorously tested for safety and efficacy and are covered by most insurance plans.
At Montgomery Gynecology, Dr. Jonnalagadda prescribes FDA-approved bioidentical hormone therapies in line with the newest ACOG and Menopause Society guidelines - giving patients the best of both worlds: hormone molecules that match the body's own, with the safety data of regulated pharmaceuticals.
Compounded "Custom" Bioidentical Hormones (Use Caution)
Compounded hormone pellets or creams are sometimes marketed as "natural" alternatives. While compounding pharmacies serve a legitimate role for patients with specific needs, compounded hormones lack FDA oversight - meaning their potency, purity, and sterility are not guaranteed. Neither the Menopause Society nor ACOG currently recommends compounded hormones over FDA-approved options for most women.
| Factor | FDA-Approved Bioidentical HRT | Synthetic Progestins | Compounded Hormones |
|---|---|---|---|
| Chemical structure matches natural hormones | ✓ Yes | ✗ No (modified) | ✓ Yes |
| FDA safety oversight | ✓ Full | ✓ Full | ✗ None |
| Clot risk (patch/gel forms) | ✓ Minimal (transdermal) | ⚠ Higher (oral) | ⚠ Variable |
| Covered by most insurance | ✓ Yes | ✓ Yes | ✗ Usually no |
| Dr. Jonnalagadda's approac | ✓ First-line recommended | ⚠ Case-by-case | ⚠ Selected cases only |
5. Evidence-Based Benefits of HRT
Proven Benefits
- Eliminates or dramatically reduces hot flashes & night sweats (most effective treatment available)
- Restores sleep quality and reduces nighttime awakenings
- Prevents bone loss; reduces fracture risk by up to 35%
- Cardioprotective when started within the timing window (the "timing hypothesis")
- Supports memory and may reduce dementia risk when initiated near menopause
- Resolves GSM (vaginal dryness, painful sex, urinary urgency)
- Improves mood, reduces anxiety, and stabilizes emotional lability
- Preserves muscle mass and reduces abdominal fat accumulation
- Slows skin collagen loss and maintains elasticity
- Reduces risk of type 2 diabetes in menopausal women
Nuanced Risks
- Small increase in breast cancer risk with combined estrogen-progestogen (roughly equivalent to drinking 1 glass of wine/day)
- Slight increased clot risk with oral estrogen (transdermal routes largely eliminate this)
- Women with history of ER+ breast cancer require individualized evaluation
- Benefits are greatest when started within 10 years of menopause onset
- Very rare: slightly increased gallbladder disease risk with oral estrogen


6. Understanding the Real Risks (And What the WHI Study Got Wrong)
In 2002, the Women's Health Initiative (WHI) published findings linking HRT to increased breast cancer, heart disease, and stroke - and the medical world reacted with alarm. HRT prescriptions dropped by nearly 80% almost overnight. Millions of women suffered through menopause without treatment for decades.
Here is what subsequent analysis revealed about the WHI's significant limitations:
- The average participant was 63 years old - over a decade past menopause - not the typical newly menopausal woman seeking treatment.
- The study used oral conjugated equine estrogen combined with synthetic progestin (medroxyprogesterone acetate) - not the transdermal bioidentical hormones used today.
- Many participants had pre-existing cardiovascular risk factors, making the heart-disease finding not applicable to healthy younger women.
- When the data was re-analyzed by age group, women aged 50–59 showed reduced all-cause mortality, reduced heart disease, and reduced osteoporosis fractures - with no significant increase in breast cancer for estrogen-only users.
"For healthy women under 60 or within 10 years of menopause, the benefits of hormone therapy outweigh the risks. This has been the consistent message of the Menopause Society and ACOG since their joint guidelines were last updated."
- Consistent with 2022–2025 Menopause Society & ACOG Clinical Guidelines
7. The Critical Timing Window for HRT
Perhaps the most important - and most underappreciated - factor in HRT outcomes is when you start. Researchers call this the "Window of Opportunity" or the Timing Hypothesis.
Stage 1 - Perimenopause (Early 40s–51): Optimal Window Opens
Hormone fluctuations begin. Starting low-dose HRT here can smooth the transition, protect cardiovascular health, and preserve bone density before significant loss occurs. Many women in this phase respond best.
Stage 2 - Within 10 Years of Menopause / Before Age 60: Prime Window
Blood vessels, brain tissue, and bone cells are still highly responsive to estrogen. Cardioprotective and neuroprotective effects are most pronounced in this window. This is the sweet spot for most women.
Stage 3 - Age 60–65: Proceed with Careful Individualization
Benefits may still outweigh risks for many women - especially for bone protection and quality of life. Requires thorough cardiovascular risk assessment. Dr. Jonnalagadda evaluates each patient individually.
Stage 4 - After Age 65 / More Than 10 Years Post-Menopause: Risk-Benefit Shift
Initiating systemic HRT for the first time is generally not recommended at this stage due to increased cardiovascular and clot risk. Local vaginal estrogen remains safe and beneficial at any age for GSM symptoms.
Key Takeaway
If you're in perimenopause or just post-menopause and are having symptoms, now is the ideal time to schedule a consultation - not in a few years. The window is real, and starting earlier generally leads to better outcomes.
8. Who Is a Good Candidate? Who Should Avoid It?
Generally Good Candidates for HRT
- Women under 60 or within 10 years of menopause with bothersome symptoms
- Women with premature ovarian insufficiency (POI) or surgical menopause under 45
- Women at elevated risk for osteoporosis or osteoporotic fractures
- Women with genitourinary syndrome of menopause (GSM) - even older women
- Women whose mood, sleep, or cognitive function is significantly impacted by hormonal changes
Situations Requiring Extra Caution or Alternatives
- Personal history of estrogen receptor-positive (ER+) breast cancer
- Active or recent blood clots (DVT/PE) - though transdermal routes significantly reduce this risk
- Unexplained vaginal bleeding (must be evaluated first)
- Active liver disease
- Untreated severe hypertension
Not Sure Where You Fall?
The only way to know if HRT is right for you is a thorough consultation with a menopause-trained gynecologist. Dr. Jonnalagadda reviews your full medical history, family history, current symptoms, and laboratory results before making any recommendation.
9. Testosterone Therapy for Women: The Overlooked Hormone
Most discussions of female HRT focus on estrogen and progesterone - but testosterone deserves attention too. Women produce testosterone in their ovaries and adrenal glands, and levels decline steadily from the 30s onward, reaching their lowest point after menopause.
Low testosterone in women is associated with:
- Significantly reduced sexual desire and arousal (hypoactive sexual desire disorder, HSDD)
- Fatigue and reduced sense of vitality
- Muscle loss and difficulty maintaining strength
- Cognitive dulling - particularly motivation and mental drive
Dr. Jonnalagadda evaluates testosterone levels as part of a complete hormonal workup and may recommend low-dose testosterone therapy - typically via cream or gel - for women with documented deficiency and appropriate symptoms. This is an area where individualized, evidence-informed care makes a meaningful difference in quality of life.

10. Your HRT Consultation at Montgomery Gynecology: What to Expect
Dr. Jonnalagadda approaches every HRT consultation the same way: with thoroughness, patience, and zero judgment. Here's the step-by-step process:
01. Comprehensive Symptom Review
Using validated menopause-specific questionnaires, Dr. Jonnalagadda documents every symptom - not just the most common ones - and scores their impact on your daily function and quality of life.
02. Full Medical & Family History
Cancer history, cardiovascular risk factors, clot history, bone density history, and family history of breast cancer all inform treatment decisions. Nothing is overlooked.
03. Laboratory Hormone Panel
FSH, estradiol, testosterone (free and total), DHEA-S, and thyroid function are assessed to establish your hormonal baseline and rule out other contributing conditions like thyroid disease.
04. Individualized Treatment Plan
Dr. Jonnalagadda selects the right hormone type, dose, delivery method, and duration based on your unique profile - not a template. She uses FDA-approved bioidentical formulations aligned with Menopause Society guidelines.
05. Advanced In-Office Technology
Montgomery Gynecology stays ahead with Clarius wireless ultrasound for accurate pelvic assessment and Lina office hysteroscopy - reducing the need for hospital visits and speeding diagnostic clarity.
06. Ongoing Monitoring & Adjustment
HRT is not a "set and forget" treatment. Follow-up appointments at 3 months and annually ensure your therapy continues to work optimally, with dose adjustments as your body changes.
11. HRT + Lifestyle: The Combination That Works Best
HRT is most effective as part of a comprehensive approach to menopausal health. At Montgomery Gynecology, Dr. Jonnalagadda integrates nutritional guidance, mental health support, and stress management alongside hormonal therapy - because hormones don't operate in a vacuum.
Key Lifestyle Pillars That Amplify HRT Outcomes
- Protein-forward nutrition: Women over 45 need more protein (at least 1.0–1.2g/kg body weight) to prevent muscle loss. HRT works with, not instead of, adequate protein intake.
- Strength training: Resistance exercise 2–3×/week is the most potent non-pharmacological intervention for bone density and body composition in menopause.
- Sleep optimization: HRT dramatically improves sleep - but good sleep hygiene (consistent schedule, dark/cool room, alcohol limitation) accelerates results.
- Stress management: Chronic cortisol elevation worsens hot flashes and undermines hormone balance. Mindfulness, yoga, and therapy are evidence-based complements to HRT.
- Alcohol moderation: Even moderate alcohol disrupts sleep architecture and modestly elevates breast cancer risk - making reduction a smart pairing with HRT.
- Calcium & Vitamin D: Essential for bone health alongside HRT. Dr. Jonnalagadda checks your Vitamin D level at your initial visit.
12. Frequently Asked Questions About HRT
Ready to Feel Like Yourself Again?
Schedule a personalized HRT consultation with Dr. Hema Jonnalagadda, MD at Advocare Montgomery Gynecology in Plymouth Meeting, PA. Most insurance accepted. Same-week appointments often available.
Book Online: healow.com/apps/practice/advocare-llc-19740
Call: 215-444-3411
115 Plymouth Road, Suite 5, Plymouth Meeting, PA 19462 · ⭐ 4.6/5 · 221 Google Reviews · Member, Menopause Society
Medical Disclaimer
This article is written for educational purposes by Dr. Hema Jonnalagadda, MD, and is intended to provide general information about hormone replacement therapy. It does not constitute personalized medical advice and should not replace a consultation with a qualified healthcare provider. All treatment decisions should be made in partnership with your gynecologist based on your individual health history, symptoms, and risk factors. Information reflects current evidence as of May 2026; guidelines evolve and will be updated accordingly.
About the Author
Dr. Hema Jonnalagadda, MD
Board-Certified Gynecologist · Founding Physician, Advocare Montgomery Gynecology · Member, Menopause Society
Dr. Jonnalagadda specializes in comprehensive women's gynecological care, with particular expertise in menopause management, abnormal bleeding, robotic minimally invasive surgery, and adolescent gynecology. She practices with a philosophy she calls "Where Innovation Meets Empathy."
⭐ 4.6 / 5 · 221 Google Reviews